Health communication
CONTENTS
Chickenpox
1. General Overview
Chickenpox is an acute infectious disease caused by the varicella-zoster virus, transmitted from person to person via the respiratory route or close contact. It occurs predominantly in children and is characterized by fever and a vesicular rash, usually with a benign clinical course. In immunocompromised individuals, pregnant women, and neonates, chickenpox may progress severely and result in visceral complications such as pneumonia and encephalitis, potentially leading to death.
Chickenpox is highly contagious, with an infection rate of up to 90% among susceptible individuals without pre-existing immunity. The disease commonly occurs in outbreaks among school-aged children.
Historical background of chickenpox:
- - In 1767, physician William Heberden described the clinical distinction between chickenpox and smallpox.
- - In 1875, Rudolf Steiner demonstrated that chickenpox was caused by an infectious agent by inoculating susceptible volunteers with vesicular fluid obtained from a patient with acute chickenpox.
- - In 1892, von Bokay observed similarities in the skin manifestations of chickenpox and herpes zoster, as well as their simultaneous occurrence within households. He therefore hypothesized that both conditions were caused by the same virus, laying the foundation for further experimental investigation.
- - In 1953, Thomas Huckle Weller proved that the viruses causing chickenpox and herpes zoster were identical by culturing the virus from both conditions. This led to the common designation “varicella-zoster virus.”
- - Subsequent studies on this virus led to the development of a live attenuated varicella vaccine in Japan in the 1970s. The varicella vaccine was licensed for use in the United States in March 1995.
2. Causative Agent
Varicella-zoster virus (VZV) is a DNA virus belonging to the family Herpesviridae, subfamily Alphaherpesvirinae, genus Varicellovirus. VZV is also known by several other names, including chickenpox virus, varicella virus, and zoster virus. It is responsible for two distinct clinical syndromes: chickenpox and herpes zoster (shingles). Primary infection with VZV causes chickenpox, whereas herpes zoster results from reactivation of latent VZV infection. VZV can survive only for a short period in the external environment.
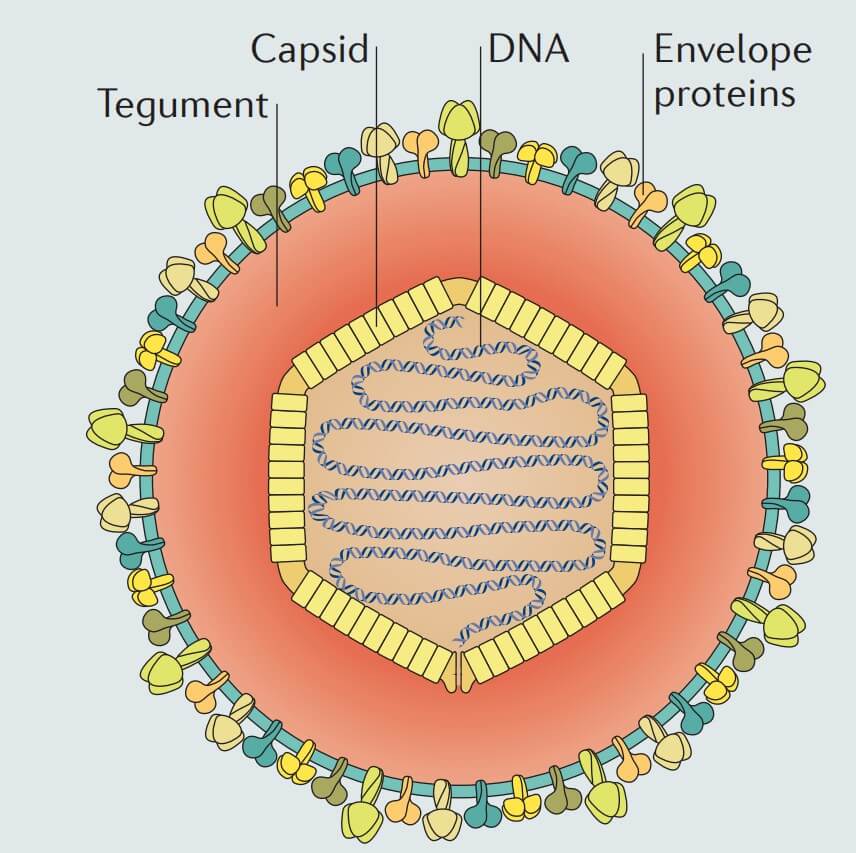
Figure 1. Structure of varicella-zoster virus
Structure of VZV:
Similar to other herpesviruses, VZV consists of four major components:
- Lipid envelope: the outermost layer of the virus, derived from the host cell membrane, containing multiple surface glycoproteins such as gB, gC, gE, gH, gI, gK, and gL. These glycoproteins play essential roles in target-cell recognition and viral entry into host cells.
- Tegument: a protein layer located between the envelope and the capsid, containing various functional proteins involved in viral replication and regulation of viral gene expression after entry into the host cell.
- Capsid: an icosahedral structure approximately 100 nm in diameter, composed of 162 capsomeres (including 150 hexons and 12 pentons). The capsid protects the viral genetic material and is involved in delivering viral DNA into the host cell nucleus.
- Genetic material: a double-stranded DNA molecule approximately 125,000 base pairs in length. This genome encodes the structural and non-structural proteins required for viral replication and pathogenesis.
3. Pathogenesis
VZV enters the body through the respiratory tract and the conjunctiva. It then replicates in the nasopharynx and regional lymph nodes. The first viremic phase occurs approximately 4–6 days after infection, during which the virus disseminates to the liver, spleen, and sensory ganglia. Viral replication continues in the viscera, and after about one week, a second viremic phase develops, accompanied by infection of the skin, resulting in the characteristic vesicular lesions.
This viremic state also disseminates the virus to the respiratory tract, facilitating transmission of chickenpox before the onset of the rash. During this phase, central nervous system or hepatic involvement may occur, including encephalitis, hepatitis, or pneumonia.
4. Clinical Manifestations
Incubation period
The incubation period of chickenpox ranges from 10 to 21 days, most commonly 14–17 days. No clinical symptoms are present during this period.
Prodromal stage
This stage lasts approximately 24–48 hours. Patients may experience mild fever, malaise, and rash, although only a minority develop prodromal symptoms 1–2 days before the rash appears. High fever may occur in adults or immunocompromised individuals. Some patients present with a preliminary rash, which precedes vesicle formation. These lesions are small, non-indurated erythematous maculopapules that persist for about 24 hours before evolving into vesicles.
Eruptive stage
In immunocompetent individuals, chickenpox usually follows a benign course characterized by malaise and fever ranging from 37.8°C to 39.4°C for 3–5 days. The hallmark of this stage is a vesicular eruption involving the skin and mucous membranes. Cutaneous lesions include maculopapules and round or teardrop-shaped vesicles, most of which are small and arise on an erythematous base measuring 5–10 mm in diameter. The vesicles appear in different stages of development: initially containing clear fluid, becoming cloudy after about 24 hours, and subsequently crusting over.
Lesions first appear on the face and neck, followed by the trunk, and then spread to other parts of the body. Similar lesions may also occur on the oral mucosa, pharyngeal mucosa, respiratory tract, vagina, and conjunctiva. Cutaneous vesicles are often pruritic. Mucosal vesicles may cause odynophagia, vomiting, dysuria, and vaginal bleeding. Disease severity is related to the number of vesicles; the greater the number of lesions, the more severe the disease. A healthy individual may develop 200–500 vesicles over 2–4 successive crops. Young children tend to develop fewer lesions than adults.
Recovery stage
After approximately one week, most vesicles crust over and later desquamate spontaneously, sometimes leaving temporary hypopigmentation at the lesion sites. Healing lesions generally do not leave scars unless secondary bacterial infection occurs.
Recovery from chickenpox usually confers lifelong immunity. In otherwise healthy individuals, a second episode of chickenpox is rare, although it may still occur, particularly in immunocompromised patients.
Chickenpox should be differentiated from other vesicular exanthematous illnesses, such as hand-foot-and-mouth disease caused by enteroviruses, herpes simplex infection, impetigo, and several other conditions.
Hand-foot-and-mouth disease may also produce vesicular lesions involving the mucosa (mouth and throat), similar to chickenpox. However, in hand-foot-and-mouth disease, the vesicles are typically smaller and distributed mainly on the palms, soles, and buttocks.
Herpes simplex lesions are usually localized to mucocutaneous junctions around natural orifices and are not disseminated over the entire body as in chickenpox.
5. Epidemiology
Source of infection
Humans are the only known reservoir of chickenpox.
Mode of transmission
The disease is transmitted from person to person through direct or indirect contact with vesicular secretions or through the respiratory route by inhalation of aerosolized particles from vesicular fluid or respiratory secretions.
Chickenpox is highly contagious; its infectivity is slightly lower than measles but higher than mumps and rubella. Approximately 70–90% of susceptible individuals without immunity will become infected after exposure in households, schools, or workplaces. Infectiousness usually begins 1–2 days before rash onset, continues throughout vesicle formation, and lasts until all lesions have crusted over, typically about 6 days after rash onset. This period may be prolonged in immunocompromised individuals.
Distribution of disease
Chickenpox occurs year-round. It is endemic in densely populated areas and may cause outbreaks during peak seasons, typically from late winter to early spring (January to May).
Historically, the most commonly affected age group has been children aged 5–9 years, accounting for approximately 50% of cases. Most remaining cases occur among children aged 1–4 years and 10–14 years.
According to a study by Huang et al. in 2022, the estimated global number of chickenpox cases and deaths was 83,963,744 and 14,553, respectively. Children under 5 years of age and older adults had the highest incidence rates.
6. Complications
Disease course
Chickenpox is generally benign in children and rarely requires hospitalization. When treated with acyclovir, patients tend to have a shorter febrile period, fewer skin lesions, and faster healing.
Complications
- Secondary bacterial infection of skin lesions, commonly caused by Streptococcus pyogenes or Staphylococcus aureus, including methicillin-resistant strains, as a result of scratching and rupture of vesicles.
- Central nervous system complications:
- Cerebellar dysfunction and meningitis, commonly seen in children, usually appearing around 21 days after rash onset and rarely before the rash. Cerebrospinal fluid may show elevated protein and lymphocytic pleocytosis.
- Encephalitis, transverse myelitis, Guillain-Barré syndrome, and Reye syndrome.
- Pneumonia: the most serious complication of chickenpox, more commonly seen in adults, especially pregnant women. It usually begins 3–5 days after rash onset and may lead to respiratory failure and hemoptysis. Chest radiography may reveal nodular and interstitial infiltrates.
- Other complications: myocarditis, corneal involvement, nephritis, arthritis, hemorrhagic manifestations, acute glomerulonephritis, and hepatitis.
- Perinatal chickenpox: occurs when the mother develops chickenpox within 5 days before delivery or within 48 hours after delivery. This form is often severe, with a high neonatal mortality rate, potentially up to 30%.
- Congenital varicella syndrome: a rare condition characterized by limb hypoplasia, cicatricial skin lesions, and microcephaly.
- In patients with HIV/AIDS, vesicular lesions tend to be atypical and may appear in successive crops over weeks to months. Initially, lesions may resemble typical chickenpox, but later they may progress to chronic ulcerative, necrotic, crusted, and hyperkeratotic lesions. This presentation is commonly observed in HIV-infected children with low CD4 counts. Interestingly, HIV-infected children with chickenpox appear to have fewer visceral complications than other HIV-infected patients with the disease.
7. Laboratory Findings
- Complete blood count: white blood cell count is usually normal, though leukopenia may occur as in other viral infections.
- Blood biochemistry: elevated liver enzymes may be observed.
Confirmatory diagnosis
- Diagnosis of chickenpox is primarily clinical and usually does not require laboratory confirmation. The characteristic generalized rash with vesicles in various stages of development in a patient with a history of exposure strongly supports the diagnosis.
- Confirmatory tests are not widely available in routine clinical practice and are seldom used. These include:
- Vesicular fluid tests: Tzanck smear showing multinucleated giant cells, PCR for detection of VZV DNA, etc.
- Serologic tests: demonstration of seroconversion or a rise in antibody titer against VZV.
8. Treatment
Principles of treatment
In immunocompetent individuals, treatment is mainly supportive and includes fever control and skin care. Anti-herpes antiviral therapy reduces disease severity and duration and is especially indicated in immunocompromised patients.
Antiviral therapy
Oral acyclovir is given at a dose of 800 mg five times daily for 5–7 days in adults. In children under 12 years of age, the dose may be 20 mg/kg every 6 hours. Treatment is most effective when initiated early, within the first 24 hours after rash onset.
In severely immunocompromised patients or in those with complicated chickenpox such as encephalitis, intravenous acyclovir is preferred, at least initially, at a dose of 10–12.5 mg/kg every 8 hours to reduce visceral complications. The treatment duration is 7 days. Immunocompromised patients at lower risk may be treated with oral antiviral agents only.
Supportive treatment
- Use paracetamol for fever reduction; aspirin should be avoided to prevent Reye syndrome.
- Administer antihistamines if the patient has pruritus at the lesion sites.
- Skin care includes daily cleansing and moisturizing of lesions, topical antipruritic agents, and prevention of secondary bacterial infection with topical antiseptics such as preparations containing aluminum acetate.
- Provide intensive respiratory support if the patient develops varicella pneumonia.
- Antibiotics are indicated when secondary bacterial infection of skin lesions or other organs occurs.
9. Prevention
Vaccination
- Varicella vaccine is a live attenuated vaccine indicated for all children older than 1 year (up to 12 years of age) who have not had chickenpox, and for adults without immunity to varicella-zoster virus. The varicella vaccine is safe and highly effective.
- Children require one dose, whereas adults require two doses. Some individuals may still develop breakthrough varicella after vaccination.
- Varicella vaccine should not be administered to children with severe immunodeficiency, including symptomatic HIV-infected children.
Varicella-zoster immune globulin (VZIG) is indicated for individuals at high risk of severe complications if administered within 72 hours after exposure to an infectious source.
Antiviral drugs may be used for post-exposure prophylaxis in high-risk individuals who cannot receive vaccination or who have passed the vaccination window (96 hours after exposure). Administration of acyclovir for 7 days after exposure may significantly reduce disease severity, even if it does not completely prevent infection.
Non-specific preventive measures
- Avoid contact with individuals with chickenpox or herpes zoster.
- Maintain personal hygiene.
REFERENCES
- Kasper, D.L., Fauci, A.S., and Harrison, T.R. (2010). Harrison's Infectious Diseases 2010. New York: McGraw-Hill Medical.
- Hall, E., Wodi, A.P., Hamborsky, J., et al. (Eds.). (2021). Epidemiology and Prevention of Vaccine-Preventable Diseases: The Pink Book, 14th ed. Public Health Foundation.
- Freer, G., and Pistello, M. (2018). Varicella-zoster virus infection: natural history, clinical manifestations, immunity and current and future vaccination strategies. New Microbiologica, 41(2), 95–105.
- McCrary, M.L., Severson, J., and Tyring, S.K. (1999). Varicella zoster virus. Journal of the American Academy of Dermatology, 41(1), 1–16.
- Huang, J., et al. (2022). The global disease burden of varicella-zoster virus infection from 1990 to 2019. Journal of Medical Virology, 94(6), 2736–2746.
- Arvin, A.M. (1996). Varicella-zoster virus. Clinical Microbiology Reviews, 9(3), 361–381.
- Galetta, K.M., and Gilden, D. (2015). Zeroing in on zoster: a tale of many disorders produced by one virus. Journal of the Neurological Sciences, 358(1–2), 38–45.
MSc. Kim Ngoc Son
MSc. Le Thi Khanh Linh